

Is It Time To Radically Rethink Our Approach To Tackling The Cross-Infection Risks Curtain Poses?
Curtains and contamination – a brief history.
Love or loathe them, since the curtain rail was invented at the turn of the last century and the first NHS hospital was opened by Aneurin Bevan in 1948, curtains have formed an omnipresent backdrop within acute care.
Essential as they have been to patient privacy, an understanding that curtains could serve as reservoirs for pathogens has been developing over several decades. As early as the 1970s and 1980s, studies began exploring the potential for various hospital surfaces to harbor infectious organisms.
However, it wasn’t until more recently, around the early to mid-2000s, that more focused research highlighted curtains as a significant source of contamination.
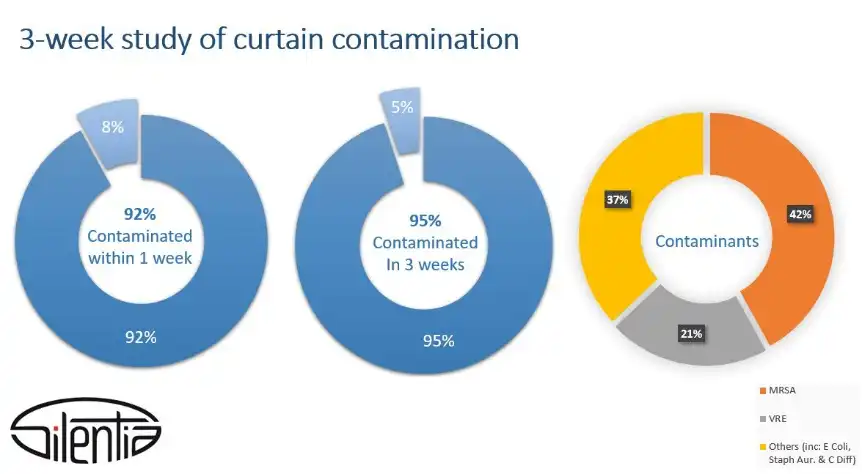
For example, a study published in 2008 in the journal Infection Control & Hospital Epidemiology1 examined hospital privacy curtains and found that 42% of sampled curtains were contaminated with VRE (vancomycin-resistant enterococci), a common healthcare-associated pathogen.
Further studies have supported these findings, confirming that curtains can often be contaminated with pathogens within a week (or even days) of being freshly hung2.
Consequently, these studies have driven changes in hospital protocols, leading to more frequent cleaning or replacement of curtains and increased use of disposable and antimicrobial curtains.
Unexpected implications of the move to disposables
The rise of the disposable curtain has had significant environmental consequences regarding increased waste, the use of plastics, and the safety of releasing antimicrobial coatings on disposal. Recycling of these products is possible but requires large amounts of energy.
There is also an impact on patient flow. Curtain changing should be done in a way that minimizes cross-contamination. Proper procedures therefore take time and involve putting the bed area out of use during changing.
Curtains pose a specific cross-infection challenge
Because curtains maintain patient privacy, they are touched immediately before and after administering nursing care.

While a nurse usually wash their hands before visiting a patient, pathogens could then be passed from the patient and back to the curtain when the nurse leaves, creating a cross-contamination cycle.
Are antimicrobial coatings the answer?
The difficulty in keeping fabric surfaces clean has led to the development of antimicrobial coatings; however, the efficacy of this approach is far from being clinically proven.
For example, a 4-week study published in the Journal of Infection Control and Hospital Epidemiology in 20123 found that one antimicrobial coating extended the median time to first contamination from 2 to 14 days. Another study showed improved results using a different layer; however, given the range of available fabric and coating combinations, more independent and comprehensive research is required to establish how effective antimicrobial coatings are, especially against more resistant pathogens. In any event, protection against pathogens likely falls far short of the minimum 6-month changing cycle many trusts practice.
There is also the possibility that antimicrobial coatings could lead to the development of antimicrobial resistance (AMR). Therefore, their use should be limited to critical applications.
National Standards of Healthcare Cleanliness – an opportunity missed?
In 2021, NHS England issued new guidelines for cleaning, representing a significant step forward in harmonizing standards4. Functional Risk Category grades areas of the hospital and cleaning frequencies are recommended for various surfaces depending on their likelihood of contamination by touching.
High-frequency touch points were identified, including:
- light switches/plastic pulls
- door handles and push plates
- bed rails
- trolleys and
- bedside locker handles

Despite curtains being a high-frequency touch point in virtually every hospital setting, they were omitted from the list.
The blind spot about curtains becomes more apparent when you compare the cleaning recommendations for each surface.
In medium-risk areas such as treatment and consulting rooms and general outpatient departments, high-frequency touchpoints should be cleaned once per week. Daily cleaning is recommended for high-risk areas such as operating theatres, intensive care, cancer, and endoscopy units.
By contrast, guidance on the cleaning or changing frequency of curtains defers to “the local curtain changing program”. It specifies a minimum cleaning/changing cycle every six months (or when visibly soiled), even in the highest Functional Risk Category.
This inconsistency in the recommended cleaning frequency of curtains versus other high-frequency touch points (daily versus twice a year) illustrates the underlying problem: it is neither practical nor financially viable to recommend that NHS Trusts change or launder their curtains every day. Instead of taking the opportunity to tackle this issue and perhaps propose alternative solutions, the new guidelines pass responsibility back to the local hospital.

Easy to clean, hard surface privacy screens
One possible and efficient solution would be to eliminate fabric surfaces in favor of privacy screens with smooth, hard surfaces which are easy to keep clean using traditional cleaning methods.
Some manufacturers, such as Silentia, offer a range of hard surface, folding privacy screens that can be wall-mounted instead of existing curtains. Well-designed privacy screens take up little wall space and feature a single touch point, such as a handle, which staff use to open and close the screen without touching the panels. Simply wiping down the handle breaks the cycle of cross-infection quickly and effectively.
Screens, which can be cleaned in situ, and without removing the patient, have a minimal impact on patient flow and bed use. Cleaning can be integrated seamlessly with the hospital’s standard cleaning routines, making managing infection control easier.
A good quality screen will have a much smaller impact on the environment as it will last a long time and can be maintained and reused.
This approach has been embraced in Scandinavian countries such as Sweden and Denmark.
In Denmark, for example, the government has not specified curtains or fabric-based screens in new build hospitals since 2013 based on the premise that all surfaces near the patient must be cleanable.
In the early 2000s, when the UK started moving from washable to disposable curtains, the Swedish chose a different path and began using folding, complex surface screens. As a result, if you walk into a hospital in Sweden today, you are unlikely to find curtains hanging in any medium to high-risk area.
Some trusts in the UK have started incorporating folding screens into new builds or refurbishments. However, curtains are still the predominant privacy solution, and many hospitals rely on the default changing policy once every six months or when visibly soiled.

Conclusion
Curtains have long been a proven source of pathogens that become rapidly contaminated.
More research is urgently needed to establish the effectiveness of antimicrobial coatings and the possible unwanted consequences for AMR and the environment.
The use and management of disposable curtains can hurt the environment and is disruptive to patient flow.
Curtains are high-frequency touch points, but cleaning or changing them daily is neither practical nor cost-effective. This may be why the issue is avoided within the 2021 NHS cleaning standards publication. As a result, infection control leads have been left with inadequate guidance on dealing with the critical risk posed by curtains.
Practical and easy-to-clean alternatives such as wall-mounted folding screens are readily available and in use in other countries such as Sweden and Denmark (as well as in an increasing number of hospitals in the UK). These alternatives should have a lower carbon footprint and are less disruptive to patient flow.
Is it perhaps time for the NHS to reassess its longstanding relationship with curtains?
For further information on Silentia privacy screens, visit www.silentia.co.uk.
Reference
1. Trillis III F., Eckstein E.C., Budavich R., Pultz M.J., Donskey C.J. Contamination of hospital curtains with healthcare-associated pathogens. Infect. Control Hosp. Epidemiol. 2008;29:1074–1076. doi: 10.1086/591863
2. Ohl M., Schweizer M., Graham M., Heilmann K., Boyken L., Diekema D. Hospital privacy curtains are frequently and rapidly contaminated with potentially pathogenic bacteria. Am. J. Infect. Control. 2012;40:904–906. doi: 10.1016/j.ajic.2011.12.017.
3. Schweizer M., Graham M., Ohl M., Heilmann K., Boyken L., Diekema D. Novel hospital curtains with antimicrobial properties: A randomized, controlled trial. Infect. Control Hosp. Epidemiol. 2012;33:1081–1085. doi: 10.1086/668022.
4. National Standards of Healthcare Cleanliness 2021, NHS England, April 2021




